
The hip bone, also known as the innominate bone, coxal bone or os coxae, is a large bone that sits in the pelvis. It is formed by the bones of the pelvis including the ilium, pubis and ischium.
The hip joint, or acetabulum, is responsible for many movements including walking, bending and crouching. It is a ball and socket joint, with the femur (top of the leg bone) sitting inside the acetabulum (hip socket).
The head of the femur is a ball-like bone structure that attaches to the rest of the femur by a section of bone called the femoral neck and sits inside the acetabular fossa. The greater trochanter is located at the top, outside edge of the femur and you can feel it when you push against the side of your hip. The lesser trochanter is located on the inside of the femur, just below the neck of the femur at the joint.
The hip socket and femoral head are both lined with articular cartilage that allows the bones to glide together easily with little friction. Articular cartilage in the hip joint is approximately 1/4" thick but gets thicker near the back of the socket where it takes most of the weight as you walk or run. It has a rubbery consistency making it able to absorb shock.
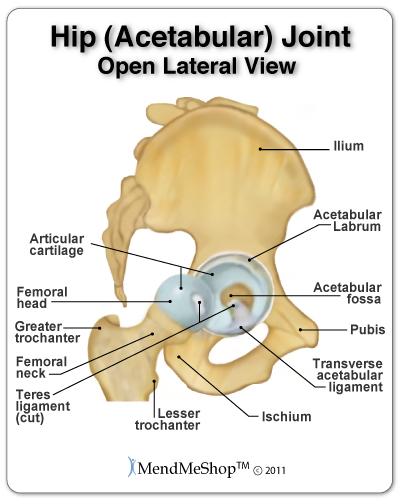
The acetabulum is also lined with a unique structure called the labrum which is a piece of fibrocartilage that forms a cup-like ring within the joint. It helps the femur sit properly in the socket, making the hip more stable. The hip joint is surrounded by other connective tissue including powerful muscles, ligaments and tendons that also stabilize the femur in the socket during it's wide range of powerful movements.
Ligaments of the hip are extremely tough and strong. Ligaments attach one bone to another and are essential for stabilizing the complex movements of the hip.
The ligaments surrounding the joint (the ischiofemoral, iliofemoral, and pubofemoral ligaments) make up the joint capsule of the hip and help control movement of the hip.


The ischiofemoral ligament attaches to the ischium of the pelvis and the intertrochanter line of the femur.
The iliofemoral ligament is the strongest ligament in the body and is an upside down "Y" shape. It starts at the anterior inferior iliac spine and the rim of the acetabulum and attaches to the anterior side of femur. It splits to join at both the neck of the femur and further down along the shaft, giving the ligament its "Y" formation. The iliofemoral ligament strengthens the hip and helps prevent the joint from hyper-extending.
The pubofemoral ligament starts at the superior ramus of the pubis and attaches to the intertrochanteric line of the femur.
There are two ligaments inside the joint capsule. One is the teres ligament, which connects the top of the femoral head to the acetabulum and contains a small artery that supplies blood to the femur. The second is the transverse acetabular ligament. It is an extension of the labrum, and is a bridge to the acetabular notch.
Bursae (plural for bursa) are flat, fluid filled sacs that function as cushions between your bones and the muscles (deep bursae) or bones and tendons (superficial bursae) to reduce friction and allow your soft tissue to slide over bone effortlessly during muscle contraction.
Bursae are lined with synovial tissue that secretes fluid that is rich in protein and collagen. This acts as the lubricant between areas in your body where friction is greatest.
There are approximately 160 bursae in our bodies, however, not everyone has the same number of bursae. Some bursae we are born with and some occur as a result of excess rubbing in a particular area. These bursae form initially to protect the area from the friction.


The major bursae in the body are located adjacent to tendons and muscles near larger joints, such as in the shoulders, elbows, hips, and knees. However, not all tendons have bursa and bursae can also form in smaller joints like your toes.
Common bursae in the hip include the deep trochanteric bursa, trochanteric bursa, iliopsoas bursa, ischiogluteal bursa, gluteus medius bursa, and the ischial turbosity bursa.
The IT band (also called the iliotibial tract, ITB or iliotibial band) is a long, thick tendon that runs from the pelvis, along the outside of the hip and femur, down to the knee. Several hip muscles connect to the iliotibial band and it's essential in stabilizing your knee while walking and running.
The iliopsoas tendon is a deep hip flexor tendon that passes along the front of the hip joint. The iliopsoas tendon attaches the iliopsoas muscle (iliacus, psoas major, and psoas minor muscles) to the femur at the lesser trochanter and is the primary hip flexor muscle.
There are four groups of muscles in the hip that are responsible for moving the leg in several directions. A listing of these muscle groups are as follows:
The Iliopsoas muscle is really a combination of 3 muscles: the psoas major, psoas minor, and iliacus. The iliopsoas muscle is the strongest flexor of the hip joint and is arguably the most important muscle group in the body. If you are doing a sit up, the iliopsoas muscle group is basically what allows you to straighten your upper body. Without it, walking is pretty much impossible.
the rectus femoris is the most prevalent of the four quadriceps muscles. The other quadriceps muscles are the vastus intermedius, vastus medialis and the vastus lateralis. All the quadriceps muscles attach to the quadriceps tendon which attaches to the knee cap (patella) - these muscles work together to bring the leg forward (hip flexion).
This is commonly referred to as hip flexor strain. Often this injury takes place at the tendon that attaches to the patella or in the muscle itself. Often the injury is a partial tear but it is not rare for a full tear to happen. The injury is caused by a forceful movement related to sprinting, jumping, or kicking and as such, is common in sports like football and soccer. The rectus femoris crosses both the knee and the hip and because of this, it is more prone to injury. Symptoms include a sudden sharp pain at the front of the hip or in the groin, swelling and bruising, and an inability to contract the rectus femoris with a full tear.
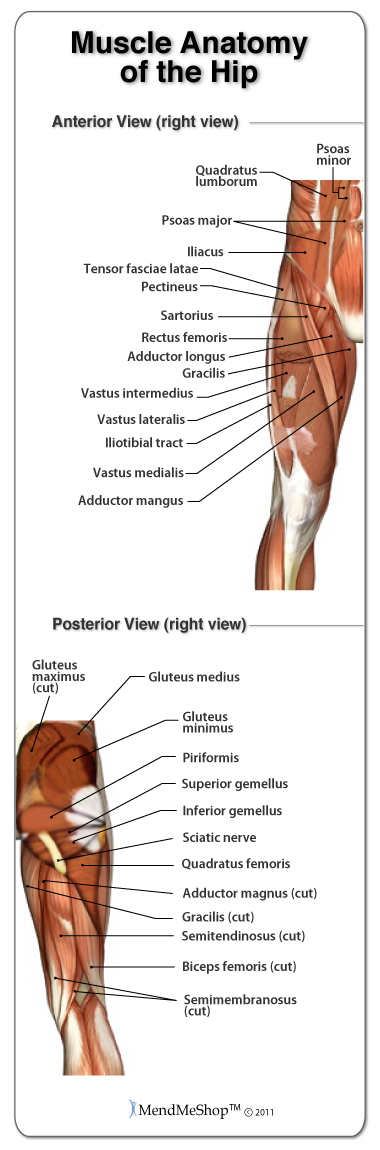
The hamstring muscles (semitendinosus, biceps femoris, semimembranosus) and gluteus maximus allow you to move your leg backward, behind your body from your hip (extension). The biceps femoris is the most commonly injured muscle in this muscle group, followed by the semitendinosus muscle. The occurrence of an injury to the semimembranosus muscle is rare.
The long head of the biceps femoris extends the hip, as when beginning to walk; both short and long heads flex the knee and laterally (outwardly) rotate the lower leg when the knee is bent.
The distal semitendinosus tendon is one of the tendons that is often considered as a candidate in the reconstruction of the ACL (anterior cruciate ligament of the knee). In such a procedure, a piece of the tendon is removed and used to replace a damaged ACL.
To be fair, I made up this name but it is really a great description of their function. The adductor magnus and adductor longus draw the leg toward the inside of the body.
Conversely, the gluteus medius, gluteus minimus and tensor fascia latae (attached to the IT band) are used to abduct your leg away from the body. The tensor fascia latae (TFL) also assists with rotating your hip inward and hip flexion.
This muscle group is basically responsible for stabilizing the hip, especially with weight bearing activities (ie. maintaining balance while carrying a child while walking or just standing).
The deep muscles of the hip include the piriformis, the obturator internus, the obturator externus, the gemellus superior, the gemellus inferior and the quadratus femoris.
Our customer service lines are open 5 days a week helping people understand their injuries and how to treat them. Simply call toll free 1-866-237-9608 to talk or place an order with one of our knowledgeable Product Advisers. They have the ability to answer questions and even put together a treatment plan for you.
Product specialists are available 9:00 am to 5:00 pm Eastern Standard Time Monday to Friday.
If any question or concern arises, call us or simply send us an email at any time (we check our emails constantly all throughout the day and night.. even on holidays!). We will respond as soon as possible.
I want to learn more about Hip Surgery & Post-Surgery Recovery
I want to learn more about Circulation Boost
I want to learn more about Ice & Heat: Which Is Better For The Hip?
I want to learn more about Trigger Points in the Hip
I want to learn more about Hip Surgery: Do I Need It?
During your recovery, you will probably have to modify and/or eliminate any activities that cause pain or discomfort at the location of your soft tissue injury until the pain and inflammation settle. The more diligent you are with your treatment and rehabilitation, the faster you will see successful results!
Please be aware that this information is neither intended nor implied to be a substitute for professional medical advice. CALL YOUR HEALTHCARE PROVIDER IMMEDIATELY IF YOU THINK YOU MAY HAVE A MEDICAL EMERGENCY. Always seek the advice of your physician or other qualified health provider before using any of our outstanding products to make sure they are right for you and your condition or if you have any questions regarding a medical condition. Always see your doctor for a proper diagnosis as there are often many injuries and conditions (some very serious) that could be the cause of your pain.
© 2025 In.Genu Design Group, Inc. Contact Us